




Interventional Care

We notice that you are visiting us from . This site only services US-based visitors. Would you like to visit the site that is appropriate for your location?

As of 30 November 2021, the United States has had 48,525,271 cases of COVID-19 leading to 779,859 deaths. In 2020, COVID-19 was the third leading cause of death in the United States, ranking only behind cardiovascular disease and cancer.1 Likely COVID-19 will also be the third leading cause of death in the United States again in 2021. The University of Washington projects estimates that by 1 March 2022, total deaths in the United States due to COVID-19 will be ~1,024,000. Receipt of a COVID-19 vaccine is the most effective preventive strategy to prevent COVID-19. This blog will review COVID-19 vaccines with a focus on the rationale for booster doses, vaccination of persons who have had COVID-19, and vaccine use in children 5 years and older.
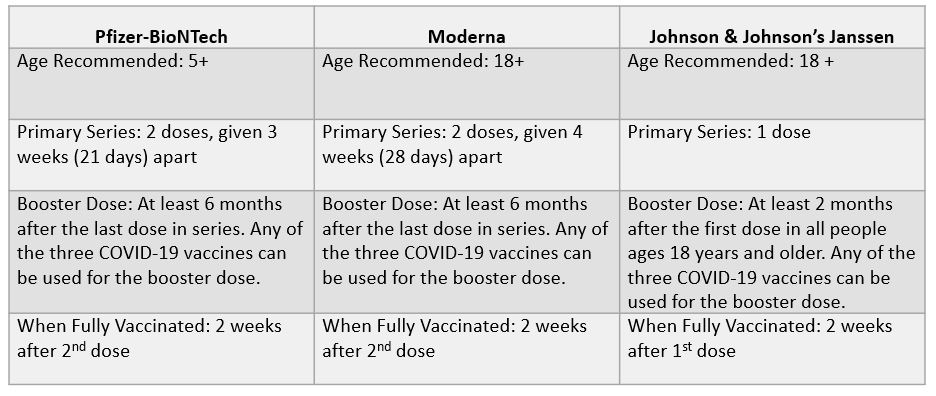
At the present time, there are three COVID-19 vaccines available in the United States either approved or authorized by the U.S. Food and Drug Administration (FDA) and recommended by the U.S. Centers for Disease Control and Prevention (CDC): Pfizer-BioNTeck (available for ages 5+), Moderna (available for ages 18+) and Johnson & Johnson’s Janssen (available for ages 18+).2 Recently, booster doses of Pfizer and Moderna were authorized for all adults by the FDA. The CDC currently recommends that all persons older than 18 years of age receive a booster dose.
Additional details on current CDC COVID-19 vaccine recommendations are summarized in the table below adapted from the CDC.
COVID-19 vaccines have been determined to be both safe and highly effective. Booster doses have been demonstrated to substantially increase the antibody levels in persons who have received a primary vaccine series. Further, two studies from Israel have both demonstrated that within two weeks of receiving a booster, the risk of developing symptomatic COVID-19 and severe COVID-19 is substantially lower. The study by Bar-On and colleagues showed that at least 12 days after the booster dose, the rate of confirmed infection was lower in the booster group than in the non-booster group by a factor of 11.3 (95% confidence interval [CI], 10.4 to 12.3); the rate of severe illness was lower by a factor of 19.5 (95% CI, 12.9 to 29.5).3 The study by Barda and co-workers showed that at least 7 days after a booster dose compared with receiving only two doses at least 5 months ago, was estimated to be 93% for admission to hospital, 92% for severe disease, and 81% (44 vs seven events; 59–97) for COVID-19-related death. Thus, all eligible persons should receive a booster dose.4
Two studies have now demonstrated that persons with natural protection (i.e., persons who have had COVID-19) have a substantially higher risk of reinfection than fully vaccinated persons. Cavanaugh and colleagues using a case-control design reported that Kentucky residents who were not vaccinated had 2.34 times the odds of reinfection compared with those who were fully vaccinated (odds ratio [OR] = 2.34; 95%CI=1.58–3.47).5 Bazio et al. using data collected from 187 hospitals reported that among COVID-19–like illness hospitalizations among adults aged ≥18 years whose previous infection or vaccination occurred 90–179 days earlier, the adjusted odds of laboratory-confirmed COVID-19 among unvaccinated adults with previous SARS-CoV-2 infection were 5.49-fold higher than the odds among fully vaccinated recipients of an mRNA COVID-19 vaccine who had no previous documented infection (95% confidence interval = 2.75–10.99).6 Thus, all persons who have had COVID-19 should receive a COVID-19 vaccine series when no longer infectious.
COVID-19 vaccines are now available for children ages 5 years and older. As with adults, COVID-19 vaccines have been found to be highly effective and safe in children. In recent months, the number and percent of children developing COVID-19 have increased. Although children, in general, have experienced less severe disease than adults, severe hospitalizations and deaths may occur.7 Adolescent hospitalization rates and mortality are substantially higher from COVID-19 compared with influenza.8 As with adults, infected children may develop COVID-19 “long haulers” syndrome with symptoms (e.g., brain fog, fatigue, etc.) lasting months.
Finally, current vaccines, in the era of the Delta variant, remain highly effective in preventing symptomatic COVID-19 and even more effective in preventing hospitalizations and deaths (CDC). Booster doses have been demonstrated to substantially increase the antibody levels in persons who have received a primary vaccine series. The U.S. now ranks 51st in the world in the level of COVID-19 vaccine coverage for its citizens (NY Times). Increasing COVID-19 vaccine uptake is crucial to protecting individuals and reducing the risk of SARS-CoV-2 transmission.
Additional Recommendations for Immunocompromised People:
Stay up-to-date on how COVID-19 vaccinations are trending in the United States here.
References:

Dr. David Jay Weber received his Bachelors of Arts (B.A.) degree from Wesleyan University in 1973, his Medical Degree (M.D.) from the University of California, San Diego in 1977, a Master’s in Public Health (M.P.H.) from Harvard University in 1985, and completed his medicine residency and infectious disease fellowship at the Massachusetts General Hospital in 1985.
He is Board Certified in Internal Medicine, Infectious Disease, Critical Care Medicine, and Preventive Medicine. Dr. Weber has been on the faculty of the University of North Carolina at Chapel Hill since 1985 where he is currently the Charles Addison and Elizabeth Ann Sanders Distinguished Professor of Medicine, Pediatrics and Epidemiology in the UNC School of Medicine, and UNC Gillings School of Global Public Health.
He serves as an Associate Chief Medical Officer for UNC Medical Center. He also serves as Medical Director of the Department of Infection Prevention UNC Medical Center. He is the Medical Director of the North Carolina Statewide Infection Control Program (SPICE), a Chair of UNC Biomedical IRB, and serves as the UNC Principle Investigator on the CDC sponsored Duke-UNC Epicenter. Dr. Weber is an Associate Editor of Infection Control Hospital Epidemiology and the Secretary of the SHEA Board. He is the Chair of the NC Health Department’s Tuberculosis Advisory Committee.
Dr. Weber has published more than 470 scientific papers in the peer-reviewed literature and more than 650 total papers and chapters. He is the Senior Editor of Mayhall’s “Hospital Epidemiology and Infection Prevention, 2020”. His research interests include the epidemiology of healthcare-associated infections, disinfection and sterilization, new and emerging infectious diseases (novel influenza, SARS-coV-2, MERS-coV, Ebola, Candida auris), response to biothreats, nontuberculous mycobacteria, control of drug resistant pathogens, immunization practices (especially of healthcare personnel), zoonotic diseases, and epidemiology of tuberculosis.


