




Interventional Care

We notice that you are visiting us from . This site only services US-based visitors. Would you like to visit the site that is appropriate for your location?

In January 2020, PDI identified five key trends in infection prevention that we believed would influence the year ahead. We weren’t wrong, but like almost everyone else, we missed the big one – the once-in-a-century pandemic that would transform everyday life around the world. While COVID-19 profoundly disrupted the course of all our 2020 trends, they remained highly relevant throughout the year and will influence how we continue to look at/approach infection prevention in the future.
Below, six members of our clinical affairs team reflect on how the pandemic altered existing trends in the infection prevention landscape, from the accelerated adoption of UVC technology to the vulnerability of folks in long-term care.
1. Layering as a comprehensive approach to infection prevention
What we thought: “In 2020, we expect the layering approach to continue to build momentum, driven by industry discussions and the availability of new technologies, such as touch-free UVC disinfection.”
The pandemic emphasized that a single strategy was not enough, and the need to adapt to supply shortages or build in redundancies to protect healthcare workers was crucial. Facilities had to maneuver and come up with innovative ways to effectively clean their environments.
In 2020, we saw broader awareness of infection prevention practices. As PDI’s Director of Clinical Affairs Debra Hagberg MT (ASCP), CIC, noted, the concept of layering expanded beyond hospital walls. “The SARS-CoV-2 pandemic has highlighted infection prevention strategies at a national public health level. Not only is the idea of layering infection prevention solutions important within healthcare, it’s heavily recommended externally as well. A lot of the world now understands the effects of compliance and/or non-compliance as it pertains to masking, social/physical distancing, environmental disinfection, hand hygiene, and contact tracing.”
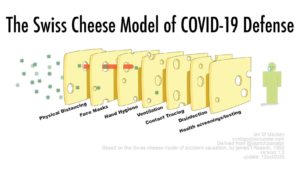
The Swiss Cheese Model – Importance of layers of protection against COVID-19
As we look ahead to 2021, layering is certainly the new “gold standard.” This approach should include an environmental cleaning program with proven practices for reducing the transmission of organisms; a robust hand hygiene program for staff, patients, and visitors, and the inclusion of new approaches such as UVC technology for even greater surface disinfection.
2. Drug Resistant Candida
What we thought: “While total HAIs are gradually decreasing in the United States, there is growing (and warranted) concern over drug-resistant strains of Candida.”
Healthcare workers have, justifiably, been focusing on managing the novel coronavirus pandemic, evolving their approach as new information becomes available. But that doesn’t mean existing threats and drug-resistant organisms, such as Candida auris, went away.
Candida auris is notoriously difficult to identify and treat, with features that may allow it to exploit the acuity of COVID-19 patients. These patients often require the placement of invasive devices and lengthy intensive care stays. While the data is rapidly evolving regarding COVID-19 and its impact on healthcare, it appears our focus on the pandemic has been to the detriment of multi-drug resistant organism (MDRO) resource allocation.
According to the CDC, the total case count of confirmed C. auris in the U.S. jumped to 1,595 on November 30, 2020 – an alarming increase of almost 70% in just over a year. Even with more robust environmental cleaning and disinfection due to SARS-CoV-2, C. auris is increasing.
Contributing factors may have been inadequate cleaning/ disinfection with the appropriate disinfectants or the use of disinfectants that don’t specifically have claims against C. auris, says Deva Rea, MPH, BSN, BS, RN, CIC, Clinical Science Liaison for PDI. “C. auris is a hardy pathogen that requires specific disinfectants – either with a specific C. auris or Clostridioides difficile efficacy claim. Another concern is that C. auris has the propensity to make durable biofilms in the environment and on devices such as indwelling catheters. Once formed, these biofilms are difficult to eradicate using traditional infection control measures.”
It’s truly a case of “insult added to injury for those working so hard on the frontlines, especially infection prevention professionals,” says Debra Hagberg. “Due to the stress and crisis mode that most healthcare facilities had to endure with surges of SARS-CoV-2 cases, the lack/reuse of personal protective equipment, the necessity of makeshift environments, and the sheer strain of trying to follow ideal infection prevention practices each time took its toll with opportunistic organism of C. auris and other pathogens.”
3. UVC disinfection
What we thought: “In 2020, these smart instruments are moving from a nice-to-have to a hospital necessity.”
Combine a novel virus, with strained raw material and supply chains, and thinly stretched and overworked healthcare/frontline workers and what you get is a perfect storm that washed over every facet of daily life. Manual cleaning and disinfecting will always be critical for removing potential pathogens, but more than ever, healthcare teams needed an extra layer of support via hands-free disinfection. Demand for UVC systems sharply increased, setting the stage for the next level of adoption for UVC as an environmental disinfection strategy.
“The SARS-CoV-2 pandemic has highlighted the need to go beyond standard cleaning and disinfection protocols to provide the cleanest possible environment,” says Tru-D® SmartUVC Director of Clinical Affairs, Alice Brewer, MPH, CIC, CPHQ, FAPIC. “A layered approach including good manual disinfection using appropriate chemicals combined with enhanced disinfection technology such as UVC is a sound strategy to ensure thoroughly disinfected surfaces.”
PDI Clinical Science Liaison Amanda Thornton, CIC, RN, MSN, agrees. “Many facilities have chosen to adopt UVC disinfection during this unusual year, integrating it into their environment of care protocols to further reduce the spread of the SARS-CoV-2 virus.”
There is increasing scientific evidence that UVC is effective at inactivating the SARS-CoV-2 virus making it an important component of a layered disinfection strategy. The International Ultraviolet Association believes that UV light can help minimize the spread of SARS-CoV-2 and is aligning with the EPA and FDA to promote best practice of this technology1.
Even though UVC technology has been used in healthcare settings for many years, it has become more widely adopted with the onset of COVID-19. So much so, that new devices have entered the market available to consumers as well. . Expect to see the trend of increased use of UVC devices to continue in the upcoming year.
4. Awareness of touchscreen contamination
Our prediction: “By the end of 2020, cleaning touch screens should be second nature.”
Touchscreen hygiene has made inroads this year. The Association of periOperative Registered Nurses (AORN) has included cleaning/disinfecting of devices prior to those devices being brought into the OR suite as part of their recently released “Surgical Attire” guideline2. The public has also become more educated and aware of the phone as a source of possible contamination and transmission of disease.
“The importance of touchscreen hygiene should not be overlooked,” says PDI Clinical Science Liaison Holly Montejano, MS, CIC, CPHQ. “Bacteria are not the only microbes found on cell phones. A study looking at viral transfer between fingers and glass surfaces found that transmission can occur, and the amount of transfer is significantly impacted by the virus strain and how recently the hands had been washed3. This is an incredibly pertinent finding in the current world of COVID-19 infection.”
With the increased use of touchscreen technology among healthcare workers the appropriate cleaning and disinfection of these devices, along with hand hygiene, will be paramount to reducing the spread of organisms. These technologies often require 70% alcohol for cleaning. To bolster compliance with device cleaning, healthcare facilities should implement a system with guidelines and staff education around appropriate cleaning/disinfection of these high-touch mobile devices.
5. CMS long-term care regulations
Our prediction: “Implementation of robust infection prevention and control programs (IPCPs) at long-term care facilities will be in top demand in 2020.”
“With upwards of 40% of U.S. COVID-related deaths occurring in long-term care facilities, the need for better infection prevention practices in LTCF cannot be overstated,” says Marc-Oliver Wright, MT(ASCP), MS, CIC, FAPIC, Clinical Science Liaison.
In many ways, these facilities were ground zero for the spread of SARS-CoV-2. PPE was in short supply and guidance from the CDC was inconsistent. Looking back, many facilities were unprepared to handle an infection crisis.4
Facilities that had proactively implemented CMS regulations without delay weathered the crisis better. But too many struggled with inadequate programs. In the first six months of the pandemic, CMS issued $15 million in fines to more than 3,400 nursing homes for non-compliance with infection control requirements5.
The lack of infection prevention training and preparedness was an unfortunate reality during the COVID-19 pandemic. More than ever, we can appreciate the need for resources, education, and fully trained professionals to prevent the spread of infection in our most vulnerable communities.
Conclusion
In the next few years, “life” will bounce back as vaccines roll out and SARS-CoV-2 is brought under control. However, its legacy will live on in infection prevention practices. The public is now more educated, UVC instruments are being added to healthcare and non-healthcare settings, and the weaknesses exposed in LTCF must be actively addressed. We didn’t predict the pandemic, but our 2020 infection prevention trends remain critical and a statement from last year’s blog definitely rings true: “new threats will undoubtedly emerge, new guidelines will come into effect, and new technologies and protocols will further the field.”
Contributions from (ABC order):
1 https://www.iuva.org/IUVA-Fact-Sheet-on-UV-Disinfection-for-COVID-19
2 https://pdihc.com/wp-content/uploads/2019/10/AORN-Guideline-for-Surgical-Attire.pdf
3 Julian, T. R., J. O. Leckie, and A. B. Boehm. “Virus transfer between fingerpads and fomites.” Journal of applied microbiology 109.6 (2010): 1868-1874
4 Long-Term Care Policy after Covid-19 — Solving the Nursing Home Crisis N Engl J Med 2020; 383:903-905 DOI: 10.1056/NEJMp2014811.


